
Recently, Biden was announced to have (likely terminal) metastatic prostate cancer. Scott Adams took that moment to announce that he did as well and that:
•Despite being a longtime critic of Biden, he deeply empathized with Biden’s plight and hoped people could show both him and Biden kindness rather than hate. He also noted he’d delayed announcing his cancer to avoid dealing with online hate and that “people are really cruel…and are going to say it’s because I got the COVID shot—there’s no indication that that makes a difference.”
•The pain from his cancer is intolerable; being on high doses of pain killers has turned him into a zombie, he now needs a walker, and he’s had to reduce his podcasts.
•He tried ivermectin and febendazole and was hopeful it would work, but it did not, and he does not want any more medical advice, nor does he want to discuss any of his cancer’s clinical history; rather he just wants to continue his podcast until his life ends.
•Because of his pain and the futility of his condition, he is deeply grateful that California allows medically assisted suicide, and he expects to be dead by the summer.
•He has often been able to visually see his future (e.g., what his future house would look like), but what he sees in the future is simply “black” so he knows he is going to die.
Note: during my life, I’ve met numerous people who had an uncanny ability to predict future events, all of whom shared that it was in part due to some degree of “psychic” foresight.
Since Scott Adams’ experience encapsulates an unfortunate but very real facet of the cancer experience, I edited his recent podcast down to just those parts:
As many know of Adams (Trump even repeatedly called him to offer support), his announcement and the bleakness surrounding it profoundly disturbed the online community and many of his previous critics, out of empathy for Scott stopped attacking him. I’ve since received many requests to comment on specific facets of it (e.g., fenbendazole and ivermectin or what’s causing these turbo cancers).
In this article, I will cover each of these and provide some context as to why I’ve taken a different approach than others when writing about cancer.
Facts Don’t Matter, Persuasion is Everything
For most of my life, the presidential election has always followed one of two courses:
•Someone skilled at influencing the public (e.g., Reagan, Clinton, or Obama) is supported by the media and wins.
•The media builds up a marginal candidate and tears down their competitors (including popular ones with populist positions) and by having everyone collapse around the chosen nominee, makes the marginal candidate appear much better than they were at the start.
When the first Republican presidential debate happened in August 2015, Trump’s odds of winning the presidency were around 1%, and most assumed he’d joined the race as a publicity stunt. As I watched the first presidential debate, I realized that:
•The 2016 primary had been set up to have all the candidates collapse around Jeb Bush so that he could be elevated to run against Hillary.
•Trump was by far the strongest candidate running, and he was also espousing populist positions that the electorate wanted.
•Based on his answer to the Rosie O’Donnell question, Trump had a degree of verbal intelligence that made him able to withstand the kill shots the media normally used to eliminate unwanted candidates.
•If Trump went after Jeb Bush, he could likely steal his spot and collapse the nomination around him.
So once the debate ended, I checked on his betting odds, saw they were way too low, and told my friends who make these types of investments that those margins would disappear in the next few days once the market caught up and recognized Trump had a realistic chance of winning.
Around the same time, Scott Adams began posting that Trump had a realistic shot of becoming president (specifically, on July 2nd he said he didn’t support Trump but he also did not support the way he was being attacked by the media, on August 5th he said there was a viable but improbable path for him to become president, on August 24th he said Trump had a more effective way to persuade the electorate than Bush, and by August 28th said Trump would win by a large margin). Since he was one of the earliest contrarian voices to say that (e.g., on August 28th another prominent pollster had given Trump a 2% chance of the GOP nomination), Adams rapidly built a following that expanded on these themes and has now grown to over a million Twitter followers.
Scott’s central message was that since he had worked as a hypnotist, he believed facts are largely irrelevant for shifting people’s opinions, and rather how they are conveyed is what matters (which to a large degree I believe is true—although I take a different approach to reaching people than Scott). In turn, Scott repeatedly identified how Trump was using persuasive messaging when sharing his talking points (e.g., his words contained poignant visual metaphors), and blended that into content creation revolving around how persuasive language and the human tendency to filter out what they don’t want to see underlies much of what happens in society.
Because of this focus, he used his framework to analyze the correct decision regarding vaccination. In the first half of 2021, he shared that vaccination had no risks, potentially protected you from long COVID-19, gave you back your freedom, would create herd immunity to COVID-19, and to varying extents belittled people who chose not to vaccinate—all of which offended many of his followers and gradually led to him being nicknamed “Clot Adams.”
Later, in January 2023, to his credit, he posted a video admitting he was wrong and the antivaxxers were entirely correct. However, framed the decision to not vaccinate as being due to one’s “luck” of habitually not trusting the government and that being correct in this one instance, rather than one of intelligence, as all the data at the time had shown vaccination to be the correct choice and every intelligent person (Adams included) who correctly analyzed that data had concluded vaccinating was the proper choice.
Given that this wasn’t entirely true (e.g., a large amount of censored data showed otherwise, historical precedent shows the US government always lies about dangerous vaccines, and many of the arguments for the vaccine didn’t make logical sense), many were understandably offended by this.
Note: another prominent online author, Emily Oster, used similar logic in a highly controversial October 2022 plea for COVID amnesty in the Atlantic.
In parallel, since the COVID vaccine has such a high rate of injuries, many prominent individuals were injured by them in a manner that could not be covered up, including many political leaders (e.g., 4 of the 48 Democrat senators had severe brain injuries specifically linked to the vaccines). All of them had promoted the vaccine, and remarkably, these severe injuries did not change their stance on the vaccine (even in the case of one Democrat Congressman who had his 17 year old daughter die suddenly from cardiac arrest).
In the midst of all this insanity, Robert Malone advocated for explaining it through Mattias Desmet’s mass formation hypothesis, which stated that under the right conditions, malignant crowd consciousnesses can take over groups of people which cause them to do completely insane and horrific things, and that the group will be incredibly resistant to any external feedback which suggesting stopping it. One of the less appreciated facets of this theory is that mass formations will inevitably die off (as they are self-consuming). Once they conclude and the insanity around them dissipates, history judges their proponents harshly.
Note: a strong case can be made that Biden suffered rapidly accelerating dementia following COVID vaccination. Since he mandated the vaccines and demonized anyone opposed to them, that is now his “legacy,” and both his political collapse and death will most likely be looked back on as yet another consequence of his horrendous decision to push the vaccines.
Early Red Flags
Given what had happened with the 1976 Swine Flu (where a “safe” vaccine the government knew was dangerous was rushed to market so it would reach America “in time” and then injured many), at the end of 2019, I was worried something similar would happen with COVID. As such, I spent a lot of time looking for ways to treat the virus so people I knew would not be forced to choose between a risky vaccine and the risk of dying from COVID.
In December of 2020, (still unidentified) hackers accessed Europe’s FDA (the EMA) and leaked some of the EMA’s regulatory documents on Pfizer’s vaccine to both the dark web and journalists. Since I was concerned about the vaccine and had a background in drug research, I read through them in detail and was left with the impression that:
•Pfizer consistently chose the available option (e.g., for its lipid nanoparticles) that was most likely to produce a viable product rather than what would produce a safe one.
•Despite going out of their way to green light the vaccines, drug regulators still raised numerous clear issues with the vaccines (e.g., fragmented rather than compete mRNA being in the vaccines or COVID rapidly becoming resistant to the vaccine), which subsequently were never publicly mentioned and to the best of my knowledge were never solved prior the vaccines hitting the market.
•Pfizer was allowed to skip a variety of critical safety studies that should have been conducted before the drugs hit the market. These included testing for genetic toxicity, cancer, impairing fertility, and autoimmune disorders—despite those being amongst the greatest concerns for this experimental gene therapy (e.g., many had pointed out the vaccines had a high risk of causing autoimmune disorders and much of this testing is typically required for gene therapies).
Note: in the EMA documents, the WHO’s 2005 position was that lipids and RNA (the vaccine’s components) were “not expected” to have genotoxicity or carcinogenicity and hence did not need to be tested for (despite regulators also noting that a component of the lipid nanoparticle was a known carcinogen). Likewise, Pfizer’s current FDA label admits that genotoxicity and carcinogenicity were never tested for.
I hence predicted that many of these issues would come to pass, and that it was quite likely many of them had been identified during clinical studies but were not reported to regulators, as “plausible deniability” of knowledge of those side effects was the only viable way to get the vaccines approved.
As such, I warned everyone I knew that the COVID vaccines might initially appear safe, but there were serious risks of long-term side effects that would take time to show up (particularly since something very similar had recently happened with the HPV vaccine). However, the moment the vaccine hit the market, I was astonished to discover that I’d greatly underestimated its toxicity and was seeing numerous patients each day who’d developed significant reactions to the vaccine they’d never experienced before. Likewise, people from around the country had begun reaching out to me to ask if the vaccine could cause you to “die suddenly” as this had recently happened to their relative (e.g., from a stroke or heart attack).
Given how much more severe the reactions were than what I’d expected, I realized the chronic issues would most likely exceed the worst case scenario I’d previously envisioned and suspected the EMA leaks rather than being hacked, came from an honest regulator who was alarmed by the gross violation of regulatory standards and what was being pushed through (but was powerless to stop it).
Note: similar in America, whistleblowers, internal Zoom recordings, and documents obtained by Senator Johnson reveal that FDA and CDC officials were fully aware of the potential dangers associated with the COVID-19 vaccines. Despite this, oncologist Dr. Peter Marks, the FDA official overseeing all vaccine-related matters, repeatedly slow-walked concerns raised by the vaccine-injured—offering empathy alongside continual excuses to delay acknowledging injuries (that were backed by credible data). He also removed two of the FDA’s top vaccine scientists who had expressed concern over the rushed approval process, discouraged the CDC from issuing even basic safety guidance (e.g., advising children with vaccine-induced myocarditis to temporarily avoid sports to reduce the risk of sudden cardiac death), and at a private conference, dismissed those questioning vaccine safety—including injured individuals he publicly claimed to empathize with—as irrational and not worth engaging.
Simian Virus 40
The biomedical industry has a longstanding problem with introducing unnatural or engineered diseases into the human population. Unfortunately, due to the copious amounts of money made from those activities, nothing has been done to address this problem for decades. As a result, more and more plagues are introduced to humanity.
A key route for this is lab research (e.g., where pathogens are engineered to make them more deadly), as the safety protocols for the labs are quite lax, and the animals these pathogens are tested on frequently will not “behave” and then infect the lab workers (e.g., by biting them). In turn, a strong case can be made that RSV, the 1971 Influenza, Lyme Disease, SARS, and COVID all originated from lab leaks (along with many others).
This issue has persisted because the bioweapons industry has faced no accountability whatsoever (e.g., Peter Hotez got a 6.1 million NIH grant to develop a SARS vaccine as a countermeasure for a lab leak and then that grant was used to fund bioweapons research at the Wuhan lab). Fortunately, Trump and RFK recently, at last, outlawed gain of function research.
Note: a few weeks ago, our new director of the NIH became aware of a safety incident at the military’s top bioweapons research facility (and one of our few facilities that studies Ebola) where one worker secretly poked holes in another worker’s protective gear (due to a lover’s spat) and hence risked exposing the entire facility to a deadly pathogen. Rather than sweep it under the rug (which is what typically would be done), Jay Bhattacharya publicly announced it and closed the lab.
A parallel issue exists with vaccines (and certain other biological products), where they will frequently be incorrectly produced and sicken the recipients. Often, this is due to the vaccine being contaminated with an infectious organism. Over the years, this has created numerous highly publicized vaccine disasters (e.g., many people got polio from vaccines that accidentally had live poliovirus in them). Sadly, because hot lots (discussed further here) are so frequent (and costly to prevent), the industry’s approach has been to sweep them under the rug (e.g., by exempting themselves from liability for poor manufacturing) rather than address them.
Since vaccine viruses require cells to reproduce, a key source of microbial contamination in vaccines is if another virus was already present in the cultured cells, and thus the final vaccine. In turn, two significant issues have been linked to contaminated vaccine cultures.
First, certain vaccines and blood products (e.g., for hemophiliacs) required either chimpanzee plasma or kidney cells, partly because it made them much more affordable, and partly because no viable alternative existed (e.g., the early hepatitis B vaccines were made by repeatedly exchanging blood between humans and monkeys to develop antibodies). Many of these were contaminated with Simian Immunodeficiency Virus (SIV), the virus most closely related to HIV.
Note: since downloading videos from Substack is a pain, every video I post here is also uploaded to this Rumble channel for anyone wishing to reuse them.
In turn, many noticed a strong correlation between these products and AIDS. For example, vaccination campaigns mirrored its spread in Africa, Haiti, and New York (and the London Times even wrote an article about it). Likewise, I had a colleague who knew a few of the participants in the original hepatitis B vaccine trials. He shared that the trial was done in a very hush-hush manner, which made his friends suspicious that they were being monitored for an undisclosed side effect and that the gay community was chosen for the initial test of the vaccine since they were less likely to have family members who would complain about any adverse effects. One of the most interesting discoveries they made was that HIV emerged shortly after the hepatitis B trials in the same cities where the Hepatitis B trials were conducted.
Lastly, for those interested in learning more, this more detailed video (a more detailed version of the above video) is the most compelling summary I have found of this entire disaster (and is discussed further here on Twitter and in this Substack article).
Note: while these contaminated vaccines caused problems, a case can also be made that a significant amount of the issues ascribed to AIDS came from other sources (e.g., the original HIV medications were extremely toxic and destroyed the immune system).
Second, rhesus monkey kidney cells (needed to grow polio and adenovirus vaccines) were contaminated with Simian virus 40 (SV40). This practice began in the 1940s, and in 1960, one of the FDA’s lead scientists discovered a previously unidentified virus that rapidly caused cancer. She attempted to alert her superiors (who were already aware of it) and was ordered not to disclose it. She did, which resulted in her losing her lab, and three years later, SV40 cells were phased out so no further contamination would occur.
Note: the inactivated polio vaccine hit the market in 1955 while the live one (which likely contained more viable SV40) did in 1961.
Numerous physicians shared that after the polio vaccines came out, cancer became more common, and the data likewise showed this.

Note: a frequently cited book, Dr. Mary’s Monkey, argued that a secret bioweapons program occurred near New Orleans, which used a hidden linear particle accelerator around 1963 to make existing viruses more harmful. Its author claimed SV40 was turned into the deadly cancer-causing virus at this time, and suggested HIV (due to SIV contamination) was accidentally created in the process as well. While this narrative is used to argue SV40 was a bioweapon program against America, I am doubtful of it as beyond many of its claims being based on inferences rather than concrete proof, carcinogenic SV40 had already contaminated the vaccine supply (and then been removed) prior to that research and it is highly unlikely a linear particle accelerator would do anything besides kill or inactivate viruses (whereas viable gain of function technologies already existed).
Turbo Cancers
The intrinsic problems with logic is that it almost always utilizes a subjective slice of reality where a desired conclusion (rather than an objective and universal one) holds true. As such, it’s quite doable to effectively argue a myriad of conflicting positions, and I often find logical “accuracy” depends upon how forcefully an argument is asserted (either by the mass media or an individual) rather than its inherent validity. For example, stringing together a series of imposing but somewhat false statements the other side is pressured into not responding to before the next one is raised is frequently an effective tactic for winning debates.
I hold a similar attitude towards therapeutic mechanisms, as while people need them, I frequently find:
•They are an educated guess rather than a definitive fit
•In many cases an effectively marketed and long accepted mechanism (e.g., depression being a chemical imbalance from low serotonin) are later disproven.
•There is often a compelling mechanism to explain things which is disregarded because it lies outside of the biochemical paradigm (e.g., many of the processes within the body governed by biophysics).
Ever since the COVID vaccines hit the market, I began hearing of people either having rapid and severe cancers (e.g., new ones, exacerbations of long stable cancers or recurrences of ones that had long been in remission). Early on I suspected this trend was real as I directly came across numerous cases almost certainly linked to vaccination (e.g., a healthy mid 20s non-smoker had a lipoma that had been stable for years which started rapidly growing immediately after a Moderna vaccine that when biopsied had an extraordinarily rare cancer only seen in older smokers that was also then found in his lungs—and then saw something similar happen to a friend’s husband).
Once the turbo cancers started appearing, we put a lot of thought into trying to explain why they were happening, and quickly ran into a dilemma—there were so many different mechanisms for carcinogenicity it was hard to say which one was the primary culprit. For instance, the NIH tried to bury an October 2021 study which showed the vaccine spike protein accumulated in cell nucleus and prevented the DNA repair—strongly arguing this was the source of their carcinogenicity.
Likewise, once SV40 was discovered in the Pfizer’s vaccines, one segment of the community (due to Dr. Mary’s monkey) began asserting that SV40 an American bioweapon that had been placed in the mRNA vaccines and the primary cause of the turbo cancers, a position disproven by the fact Moderna did not have SV40 but still caused turbo cancer. Furthermore, while SV40 was known to slowly cause cancers, the vaccine cancers we saw were rapid (and have already caused a massive spike in cancer rates that is much faster than what was seen after SV40) and the SV40 sequences in the vaccine were not the parts of SV40 thought to be primarily responsible for causing cancer.
Note: one of the most common ways positions critical of the establishment get disproven is by associating them with extreme and questionable ideas so that the valid positions can be lumped under the same “conspiracy theory” umbrella and easily dismissed. In some cases I think this is deliberately done to sabotage a threatening counter-narrative but in many other cases I believe it’s done because one-upping another person’s theory with an even darker one has long been an effective way to attract an audience. In the case of SV40, I’ve found people will talk about the problems caused by the SV40 virus, and then state “SV40” (rather than SV40’s promoter) is in the vaccine, thereby implying but not explicitly stating the virus is there.
The day the sequence of DNA plasmids contaminating the Pfizer vaccine became available (due to Kevin McKernan independently DNA sequencing the vaccines) my attention was immediately drawn to the presence of the SV40 promoter being in their DNA. My first thought was that this explained why they are causing cancer (and hence that I needed to write an article about it), which was followed by “since the SV40 promoter is one part of the SV40 virus, its effect may not be the same as that of the entire virus” so I need to figure out exactly what it does before taking a public position on this and inadvertently spreading misinformation.
Building Vaccines
Many things within biology rely upon enzymes, which are analogous to computer programs, that in concert, are calibrated to create all the molecular changes necessary for life. Much of biotechnology has revolved around identifying key enzymes (or gene sequences) from across the globe which can be creatively combined together to create a desired end product (e.g., PCR tests use a bacterial enzyme which rapidly copies existing DNA, thereby making enough of it for faint traces of it—such as from a viral infection—to be detected).
For the mRNA vaccines to work, a massive amount of custom mRNA had to be produced, which was then delivered into cells and able to persist long enough for their protein product (the spike protein) to be made in amounts sufficient to elicit a lasting immune response.
Each of those represented a major challenge, most of which had not been solved (especially in a manner that was safe). Worse still, there was incredible pressure to get a vaccine quickly to market (e.g., regulatory standards had temporarily been loosened to ensure a vaccine that could end the pandemic was produced, once the initial ones were approved subsequent vaccines from other companies would be unlikely to sell, and COVID was on its way out so the need for them would disappear entirely before long).
As such, the solution chosen for COVID-19 was:
•Have Operation Warp Speed pre-pay for a myriad of vaccines (so that the financial risk of investing in developing a vaccine was removed and enough of which ever vaccine that passed clinical trials to America would be made available).
•Shield the manufacturers from any liability for injury so safety concerns did not need to delay finding a way to create vaccine efficacy.
•Create a very low bar for vaccine approval (an Emergency Use Authorization).
•Go full-bore with each existing biotechnology that could solve each of those problems and ignore any potential issues from overusing it.
Specifically:
•In the initial clinical trials, PCR was used to replicate vaccine mRNA. Since this could not be scaled up sufficiently to produce billions of vaccines, after the PCR based vaccine got approval, a different untested process was utilized. In it, synthetic bacterial plasmids (DNA) were given to bacteria, which were then reproduced and killed to extract their plasmids, which were then turned into mRNA with an enzyme, while in parallel, steps were taken to eliminate everything besides the synthetic mRNA from the final product. However, this rushed purification was not done correctly, and as a result, we were able to detect the plasmids in the vaccines and reverse engineer what had been done from their genetic sequence.
•To ensure high amounts of plasmid DNA were turned into mRNA, promoters (DNA sequences which tell other enzymes to begin that conversion) such as T7 were needed.
•After extensively studying it for its carcinogenicity, researchers eventually realized one of SV40’s key properties was a robust promoter that rapidly reproduced its RNA within cells. That discovery led to its utilization in biotech because a robust promoter was often needed. In turn, when Pfizer was looking for a robust promoter, they used SV40s to increase the likelihood of their vaccine succeeding.
•While nowhere near as carcinogenic as the SV40 virus, the SV40 promoter had a few key issues, such as directing foreign DNA into cellular nuclei (hence increasing the risk of DNA alternations) and binding the primary protein the body uses to prevent cancer.
Note: other components of the vaccine also made it able to change your DNA.
•Since the body would rapidly break down mRNA, pseudouridylation (turning mRNA uridine into pseudouridine) was utilized as pseudouridylated mRNA resists degradation. Since synthetic pseudouridylation is largely a random process and still poorly understood, a decision was made to “overdo” it so that enough mRNA could be pseudouridylated to ensure the vaccine worked (despite this mRNA also being more toxic and immune suppressing).
Note: a second part of the SV40 virus (the PolyA tail, was also used both to prevent mRNA degradation and to enhance mRNA production).
•To ensure that whatever antigen was finally produced could elicit a strong and relevant reaction, the most reactive part of the virus (the spike protein) was chosen, despite this also being the most toxic and rapidly mutating part (hence, COVID variants quickly emerged that were immune to the vaccine).
Because of all of this, the mRNA vaccines got approved but also had a litany of issues we are gradually discovering, such as its spike protein persisting in the body for a multiple years after injection (most likely due to pseudouridylation but possible also due to plasmid DNA integration leading to cells also producing the vaccine).
In short, there are so many different problems with the vaccine that it’s quite challenging to know what the actual mechanism of carcinogenicity is. For this reason, I’ve repeatedly discussed this topic with Dr. Ryan Cole, someone I consider to have the rare combination of being very intelligent and capable of seeing the whole picture without bias, who due to his background with cancer, has extensively studied the question. Cole’s opinion (and hence mine) is that the primary issue is chronic immune suppression induced by the vaccines (which causes cancer, as typically the immune system contains and eliminates cancers), which is then compounded by all the other carcinogenic effects of the vaccine.
Note: much of this immune suppression is due to immune burnout (from chronic overstimulation by months to years of continual spike protein production). For example, a 2022 paper (and many that followed) showed the vaccines eventually triggered an IgG4 class switch and most recently, a comprehensive Yale study of the immune alternations and spike protein persistence seen years after mRNA vaccination.
Ivermectin, Febendazole and Mebendazole
Note: since febenazole is only approved for animal use, some practitioners use it and others do not (instead only using mebendazole).
After Scott Adams posted his story, many commenters (who likely had not listened to the video) implored him to try ivermectin, fenben, and mebendazole. The top comment on the thread came from Dr. Makis, a leading proponent of that protocol which stated:
Ivermectin and Fenbendazole combination has about a 75% response rate across all cancers. While that’s better than any cutting edge cancer treatment out there, I wish it was 100%. It isn’t.
There is no way to predict who will respond and who won’t.
Note: this was followed by examples of how the protocol could be done incorrectly (e.g., sometimes higher doses of febendazole or mebendazole were needed, the wrong form was taken, or fats were not eaten concurrently) and then:
You can’t give up if it doesn’t work on the first try, that’s the key.
Scott, I hope you beat this cancer and my doors are open to you and anyone else should you wish to try again.
Since that time, Scott Adams has pinned this on his page:
Note: one of the most challenging things cancer patients face is everyone cathartically projecting their anxiety onto the cancer patient and bombarding (or pressuring) them with unsolicited medical advice. For this reason, we sometimes advise patients to restrict their open avenues of communication and designate a trusted friend or relative to field those inquiries.
As Pierre Kory has the most experience with this subject (e.g., he and now three others in his practice have been treating cancer patients for the last year and a half) and I find that he’s relatively objective in his assessments (e.g., he greatly overextends himself to find ways to get patients better but will frequently share that something he’d hoped would work did not) I queried him on this.
He stated that they’re in the process of tabulating the data to get an exact figure, but his experience (using the correct dosing of the drugs) has been that:
•10% of patients have a dramatic response to ivermectin and mebendazole.
•15% have no response.
•75% may have a response, but it’s very difficult to say because they are on many other concurrent conventional and alternative therapies, and often the result is not a remission but rather a halt of cancer progression (which is still often quite monumental).
•We still have no idea how to predict which cancers will respond to it.
•At high doses, ivermectin will cause visual toxicity, so you can’t solve the issue with higher doses.
Note: highlighting his objectivity, while Pierre Kory was once the leading advocate for ivermectin to treat COVID, he no longer does as the newer variants don’t respond to it (whereas vaccine injuries do because the vaccines used the original spike protein).
In my case, I learned about fenben (and then mebendazole) roughly a decade ago, and from consulting colleagues, found it sometimes worked, but in many cases recurrences followed. For these reasons, over the years, my network rarely used it, and I hence refrained from discussing the topic as I had no direct experience with it. Recently ivermectin got added into the mix in the and people began extensively discussing the miraculous cancer cures some combination of those drugs created. Because of that, I began to hear much more about it and:
•Periodically came across people in my community who’d used them without success.
•In the success stories I heard, enough other things were in the mix, I could not say if it was what worked.
•Both me and the Vigilant Fox received messages from people who’d taken it, it hadn’t worked and they were now desperate for our help because their cancer had metastasized and they didn’t know what to do.
•I came across one case where a widely seen success story attributed to this protocol was exaggerated and did not accurately reflect the patient’s medical records.
•A few doctors have shared with me that generally speaking, a positive response to ivermectin will be seen within the first 30 days, but it normally takes about 4 months to know if it will work (as the initial positive response can be followed by a treatment failure or a miraculous recovery). As such, many testimonials online that are based off only the first month of results are highly misleading.
Because of this, I feel that this protocol is something worth trying as it relatively safe, very affordable and accessible, and has a small chance of making a dramatic improvement that spares you from the nightmare of going through chemo and radiation therapy (hence making it dramatically better than most of the conventional options). However, I also believe the rampant use of miraculous testimonials to promote it (rather than consecutive cases or trials that also show the treatment failures) has created a massive inflation of its efficacy and individuals choosing to eschew other treatments who then either die or lose much of their faith in unconventional treatments.
Note: the only dataset I’ve come across where some aspect of this protocol has a high rate of success has been from people using topical ivermectin in conjunction with DMSO (discussed further here). In addition to a few success stories from readers, one doctor has tried this in his practice and reported topical DMSO-ivermectin treated a metastatic colon cancer, appeared to have a good response in 5 prostate, 1 breast and 1 ovarian cancer that had not metastasized (e.g., 4 PSA’s normalized), and may have helped a brain cancer (but for those 8 cases, conclusive data through imaging is still being awaited). Additionally, 30 or so other patients were recommended the protocol, but no followup was possible with them (due to his practice being both in person and a Telehealth, and those 30 being Telehealth rather than in person patients), so it is not known if they did the protocol or it worked for them.
Treating Cancer
One of the immensely challenging things about treating cancer is that to some extent what each cancer responds to differs and typically, there are a variety of precipitating factors in the background that cause cancers (e.g., certain nutritional deficiencies, traumatic emotions, excessive unopposed estrogen, systemic disturbances of the body’s microbiome, chronic infections such as those within root canals, poor sleep overwork and chronic stress, or impaired detoxification pathways).
Because of this, while certain treatments have a rather broad spectrum of applicability to cancers (e.g., IV vitamin C), the specific treatments people need greatly vary and the specific protocols we give people often greatly differ. Conversely, the only thing I know that works consistently is using complementary therapies to mitigate the effects of a conventional treatment (e.g., ultraviolet blood irradiation for chemotherapy or DMSO for radiation therapy) or potentiate them so lower doses are more likely to elicit a cure.
Note: generally speaking, turbo cancers from the COVID vaccines are more challenging to treat than standard cancers. Likewise, early cancers (e.g., prostate cancer) are much easier to treat than late ones, but unfortunately, we frequently instead see patients after they have exhausted all treatment options or allowed a contained cancer to progress to the metastatic stage. As such, the specific protocol we chose also must be calibrated to the disease progression.
Unfortunately, conventional therapies all have significant downsides too, the specific one chosen (especially a chemotherapy drug) isn’t always the right one to use for a cancer, and even when they work, the patients still feel awful from their side effects (but still often are continued on the drugs by their oncologist to ensure there is not a remission).
Because of all of this, any blanket position I take will inevitably be wrong for some of the people here (e.g., sometimes I press people who do not want to do chemotherapy to do it because I know they will die otherwise whereas in many other cases I do all I can to get people to stop doing it because I know it’s killing them) and it’s hence complicated for me to give any definitive guidance on the topic.
As such, the only alternative cancer therapy I have discussed in detail here was DMSO mixed with hematoxylin (something I consider to be relatively safe and has one of the highest efficacies amongst all of the alternative cancer treatments I’ve looked at). However, I only promoted it because I was able to correspond with a doctor who quietly spent 15 years utilizing and refining the therapy so that he could determine precisely how effective it was and when it worked or did not work so that if it were ever publicly promoted people would know when/where/how to use it rather than abandoning it because it failed to meet their (erroneous) expectations. Likewise, while he greatly wanted me to promote it, again and again he stipulated that I could only do so if I accurately presented his data, as all he wanted, was for it to get the best chance it could to see the light of day.
For instance, while D-hematoxylin is very helpful for local prostate cancer (and free of the side effects seen with conventional treatment), we don’t know if it has any value in metastases as beyond the near death case Jim McCann treated (which we lack any concrete information on) the only data on this came from Tucker’s original series of recurrent cancers, which included two prostate cancer patients (both of whom had received no other cancer therapies). In the 50-year-old, with vertebral metastasis, they had a remission, while in the 73-year-old with a generalized metastasis, their tumor regressed for 4 months after which they died—all of which is quite encouraging but not enough to claim is a cure. Additionally, while many cancers (e.g., leukemias) have an excellent response to it, bone metastases (which characterizes metastatic prostate cancer) do not.
Note: one of the major challenge in treating cancer (especially advanced ones) is that patients can lose the will to live, and for many natural cancer therapies (e.g., this is the case with D-hematoxylin), unless the patient genuinely wants to live, the therapy often does not work. This is extremely frustrating to encounter (especially if you heavily invest your energy into healing the patient), and I now believe this is a form of extreme depression triggered by extreme fluid stagnation (that affects the interstitial fluid of the body). One of my major regrets was that I did not figure this out earlier, and I now wonder if one of the key reasons why DMSO improves some of the most challenging symptoms of cancer is because it improves that fluid stagnation.
Palliative Cancer Therapies
One thing that’s very difficult to appreciate about advanced cancer (unless you or a loved one has experienced it) is how miserable the whole process can be, how severe the pain is, or what it is like to know there is an inevitable death in the near future, that you can do nothing about. On one hand, this helps to illustrate why some chose to commit suicide, while on the other hand, it helps to provide important context to Lupron’s approval.
Note: Lupron is a fairly dangerous drug which (often permanently) shuts down the body’s production of sex hormones. At the time of its approval, the FDA had grave reservations about it, but eventually approved it as a palliative (symptom improving) treatment for advanced prostate cancer because it yielded comparable results to DES (a now banned estrogen analog). Due to its toxicity and poor efficacy, urologists initially did not want to use it, but eventually did once they started receiving massive kickbacks for doing so. Following that, its lucrative market was expanded into gynecologic issues (where it severely injured many women), and then to children (initially to make them grow taller, and then once that failed, to delay puberty for sex changes)—all of which is discussed here.
Cancer pain is often incredibly challenging to treat (e.g., proficiency in managing it is a key skill physicians must develop when seeking board certification in the subspecialty of pain medicine). In turn, it’s often so severe that the general restrictions on opioids are typically lifted for it (e.g., fentanyl is frequently used to treat advanced cancer pain—but in 10-20% of patients, their pain is severe enough that even potent opioids can’t address it).
Since DMSO has a rather unique mechanism of treating pain, it is often able to treat a wide range of challenging pain conditions that nothing else works on (discussed further here) and to do so without the myriad of side effects accompanying strong opioid use (e.g., drowsiness and mental fogginess). In turn, many over the years have found it provided incredible relief for metastatic cancer pain. In addition to many compelling anecdotal reports, a few studies have shown this too:
•A 1967 study gave two older patients with cancer pain DMSO, one of whom had an excellent response to treatment and one who had a good response.
•A 1967 study found that of 7 patients with metastatic cancer pain, DMSO gave 2 a full remission and 2 a partial remission.
However, most of the palliative studies with DMSO were done in conjunction with baking soda (which has a bit of data to support its use as an alternative cancer therapy and is offered by a few facilities). These studies (discussed further in this article and authored by a doctor who now teaches at a Los Angeles medical school) showed rather remarkable improvements in the suffering patients with advanced cancers experienced.
Specifically:
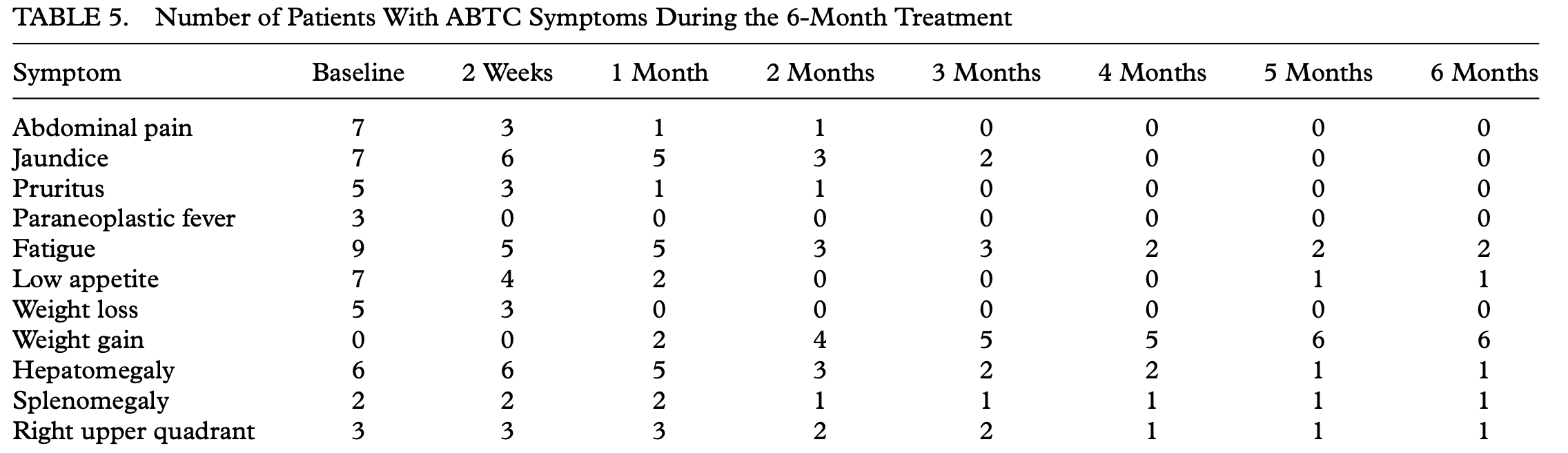
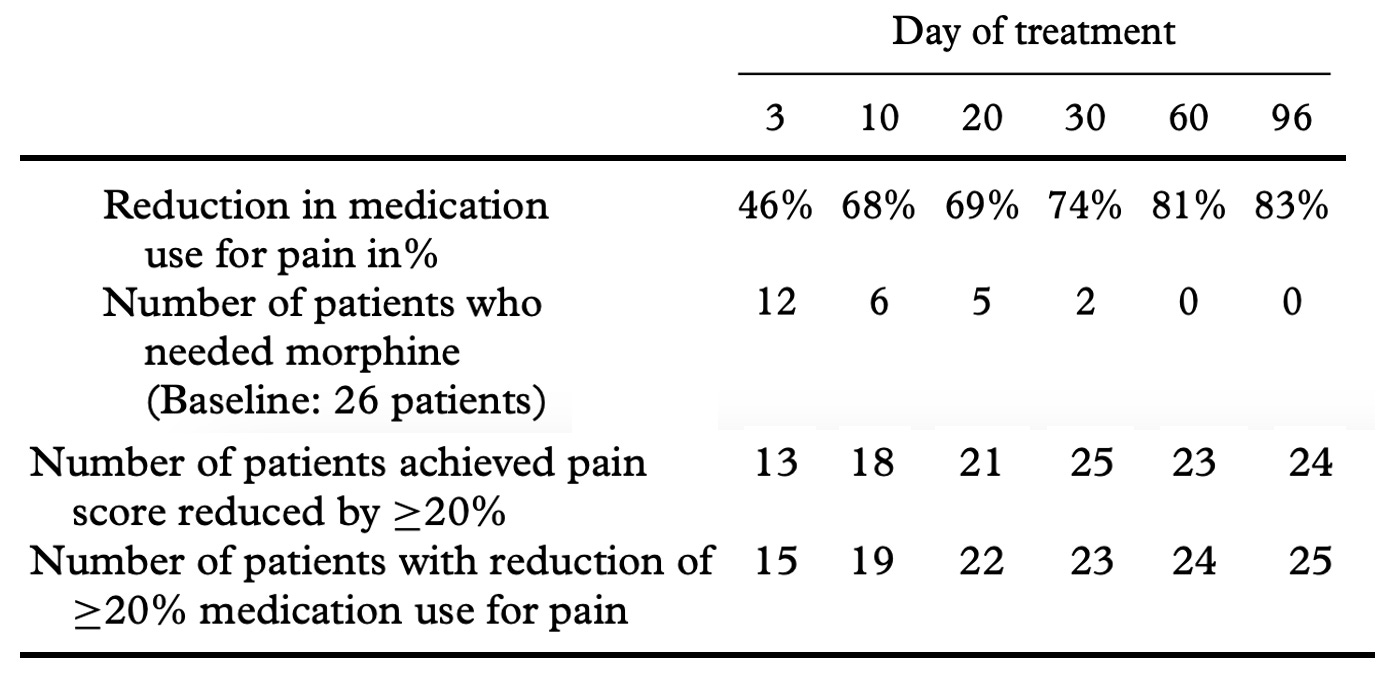
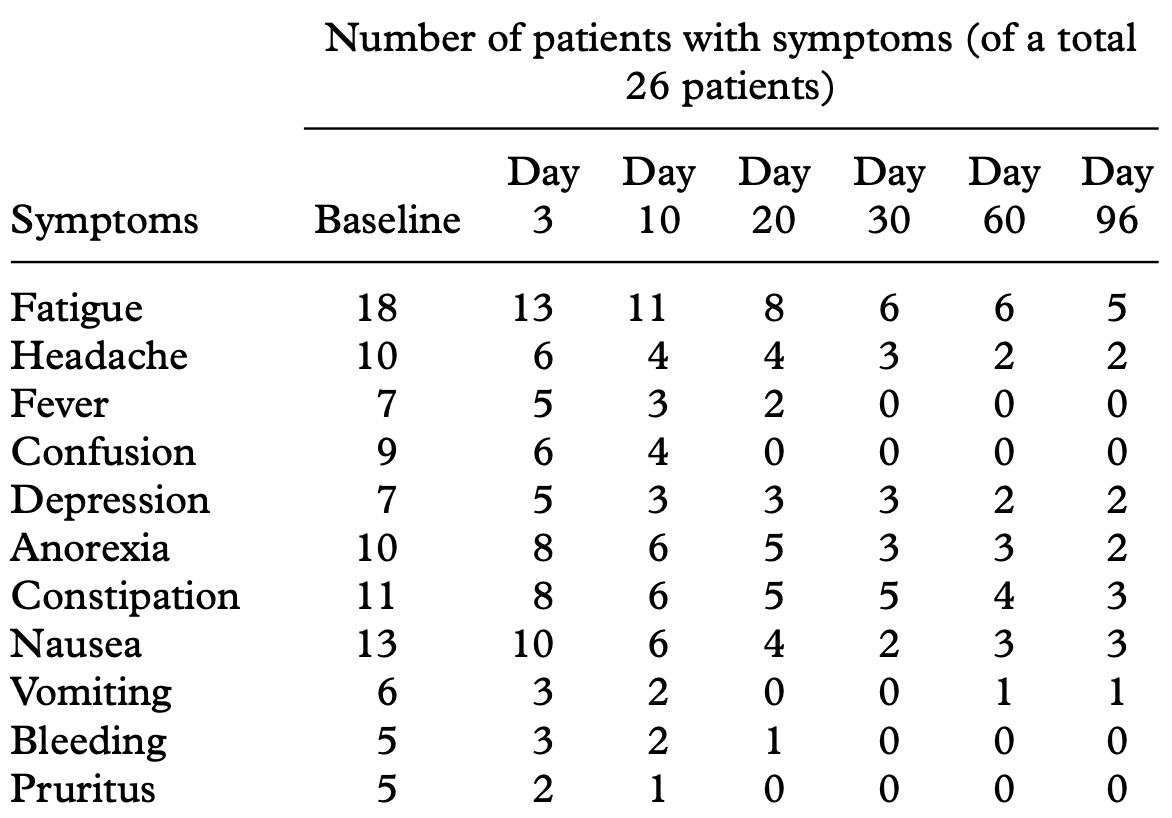
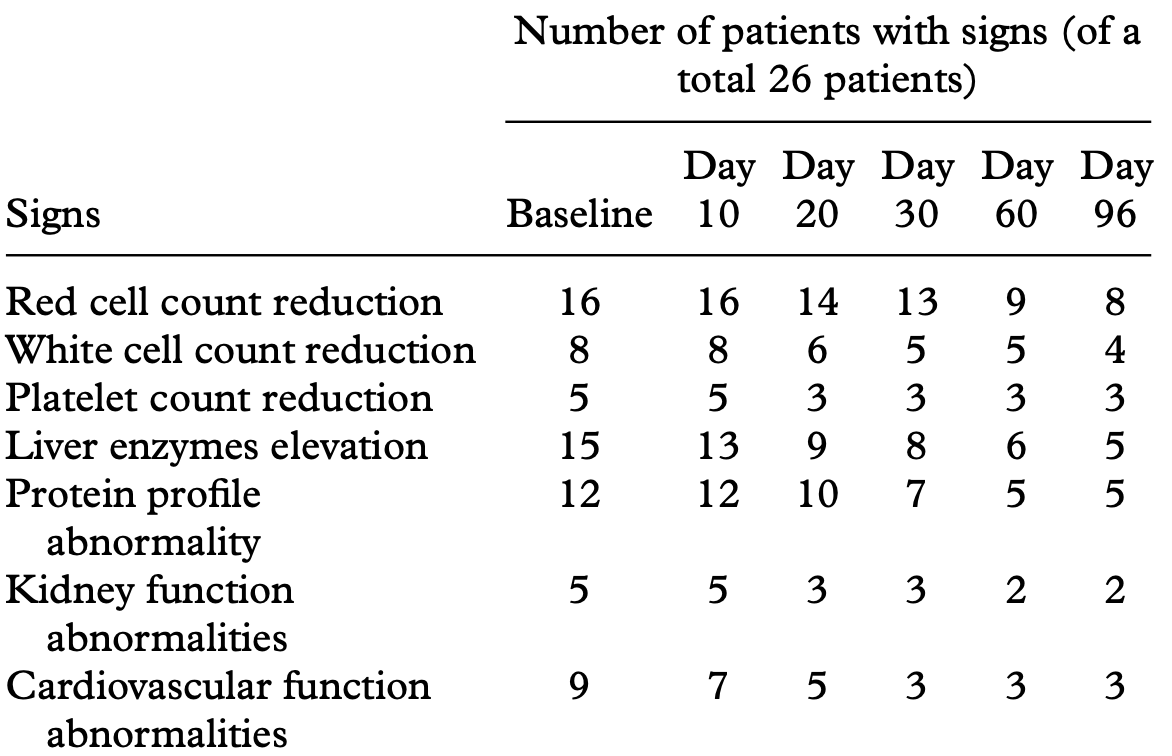
•A 2011 study gave IV DMSO combined with sodium bicarbonate (baking soda) to patients with metastatic prostate cancer. It found that after 90 days, the patients treated with this mixture showed significant improvement in symptoms (e.g., pain) and no significant side effects from the treatment. Other major improvements were also seen:
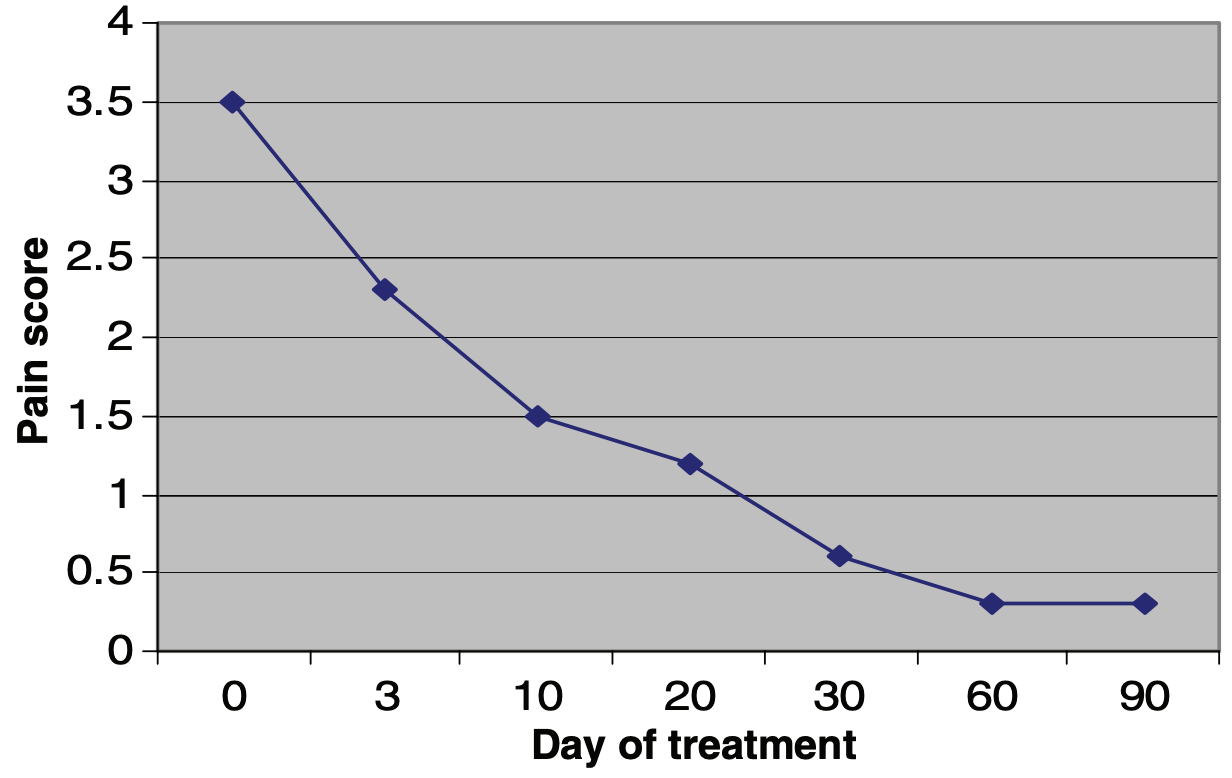
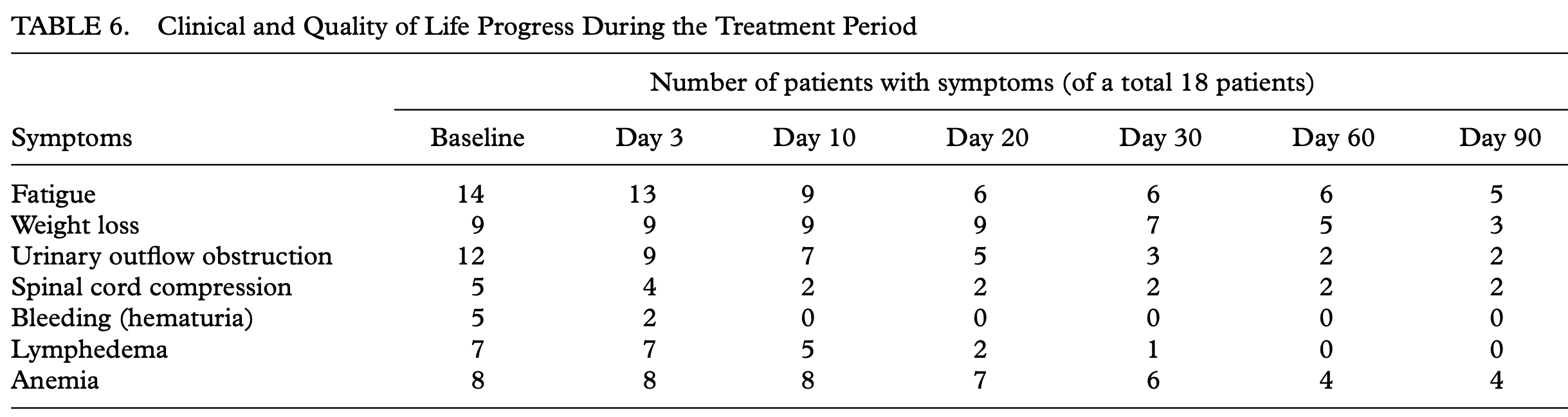
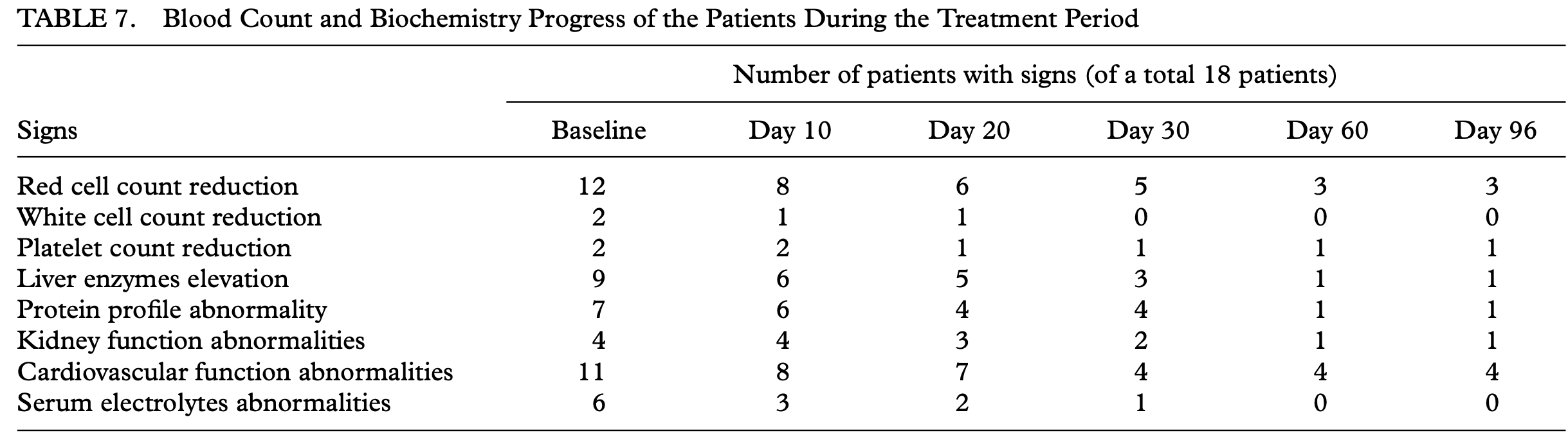
Note: given the symptoms that improved, I suspect many others did as well (but were not measured because they were outside the study protocols).
•In a follow up study, nine patients with advanced biliary adenocarcinomas (which are typically fatal) were given continuous infusions (lasting most of the day) 5 days each week that consisted of DMSO along with sodium bicarbonate, magnesium sulfate, potassium chloride and S-adenosylmethionine. After two weeks of treatment, the patient’s abdominal pain decreased by over 50%, their quality of life had improved, their biochemistry demonstrated that their disease had stabilized, and there were no significant adverse effects.

•Finally, in a 2011 study of 26 patients with severe refractory pain from advanced cancers, DMSO sodium bicarbonate infusions were given once a day for 10 days with 2-day breaks from the cycle. This was a safer and more effective method of pain control that also improved the patients’ quality of life, reduced the side effects of chemotherapy, and possibly increased their length of survival.
Additionally, this 2010 paper explores the mechanisms behind DMSO’s ability to treat intractable cancer pain, such as its ability to address membrane hyper-excitability (e.g., through suppressing NMDA and AMPA-induced ion fluxes, which are linked to central pain sensitization and may explain why DMSO effectively treats complex regional pain syndrome).
Note: one of the key reasons I feel comfortable promoting DMSO is because you normally quickly know if it’s helping (rather than having to wait months for a cancer change), it’s not catastrophic if it doesn’t work (e.g., as nothing was being done with the issue to begin with), and there is negligible cost or risk in using it (provided its used correctly), so when DMSO doesn’t work, it creates very little ill-will. Fortunately, that’s quite rare (around 85-90% of people respond to its common indications), hence an acceptable trade-off to ensure those who can benefit from it do.
Conclusion
I have long believed that when the truth is on your side and you can articulate it clearly, it will ultimately be heard. Since many of the forces we are working against (e.g., the pharmaceutical and agrochemical companies that stand to lose billions from MAHA) are so monolithic and cutthroat, for us to prevail, we must harness the power of our truth.
To do that, we must focus on advancing things we know to be true and, regardless of how tempting it is to do so, not exaggerate them, as the moment we do, it breeds seeds of distrust that fracture our movement. Many of the things we are dealing with are so upsetting and hard for many to conceive could ever be occurring that there is a natural tendency to assume everything we’ve been exposed to is a lie. However, while that is to some extent true, that same skepticism needs to be extended to new ideas, as every narrative is malleable, and many will promote ideas that sound nice but aren’t necessarily true (e.g., the SV40 virus being the cause of the wave of cancers we are seeing now).
Fortunately, despite the obstacles we face, MAHA is continuing to make incredible progress inside the government, which is on a scale completely different from anything I’ve seen in my lifetime or even thought was possible. For example, this physician was recently promoted to deputy director (second in command) of the FDA. After hearing her recent talk (which gives an inside look at the FDA), I was astonished that someone like her would ever have that role there:
Likewise, today the first MAHA report was released, which in our eyes is a monumental document as:
• It is the first time the Federal Government has ever officially acknowledged many of the major health issues facing our country (e.g., nine of its authors were cabinet-level officials including six secretaries).
• It is a surprisingly comprehensive summary of many of those issues (and as such, I would strongly recommend looking through it if you have time).
Finally, despite it being incredibly difficult to get anything done at the FDA, MAHA’s work to get the COVID vaccines repealed is continuing to move forward. As a result, we saw this wonderful message from the same fellow who just spent the last four years trying to force everyone to vaccinate:
This is immensely encouraging, and I now feel a real degree of improvement in our health is guaranteed. However, because so many things need to get done (e.g., making real cures for cancer available rather than stonewalling them as the FDA and NCI have done for decades), our available resources aren’t enough to get to all of them. For this reason, it is critical that our focus does not get diverted into polarization and division (which the corporate media is now trying to promote as MAHA is threatening the major businesses that sustain themselves through poisoning us), and likewise, for each of us to do what we can to support these efforts.
For example, recently a MAHA contingent visited the Capitol. One attendee, Sherri Tenpenny (who writes on Substack, recently authored a phenomenal book on vaccine corruption, and has done an incredible amount of work for the vaccine safety field over the decades) shared some poignant observations of what is happening there right now:
I’ve waited for something like this my entire life and I feel incredibly grateful that I can be part of it and to each of you who has helped give me the voice I have.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.